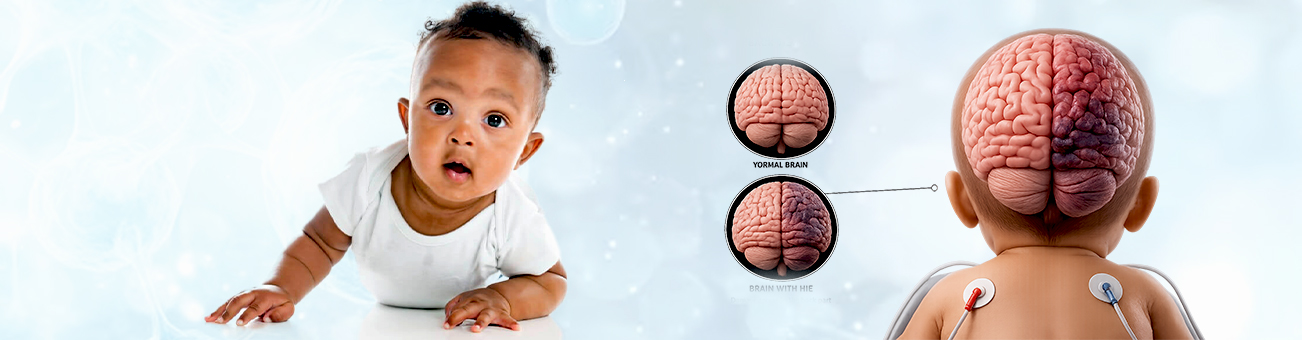
Diagnosing hypoxic-ischemic encephalopathy (HIE) promptly is crucial for initiating appropriate interventions to minimize brain damage and improve outcomes. The diagnosis involves a combination of clinical assessment, laboratory tests, and advanced imaging techniques. Given below are the key components involved in diagnosing HIE:
Clinical Assessment
Apgar Scores:
Apgar scores are assigned at 1 and 5 minutes after birth based on heart rate, respiratory effort, muscle tone, reflex irritability, and color.
Low scores (especially if prolonged) can indicate distress and the need for further evaluation.
Neurological Examination:
Alertness and Responsiveness: Assessing the infant’s level of consciousness, ranging from alert to lethargic or comatose.
Muscle Tone: Checking for hypotonia (reduced muscle tone) or hypertonia (increased muscle tone).
Reflexes: Evaluating primitive reflexes such as the Moro reflex, sucking reflex, and grasp reflex.
Seizures: Observing for any seizure activity, which is common in moderate to severe HIE.
Laboratory Tests
Blood Gas Analysis:
Arterial Blood Gas (ABG): Measures pH, oxygen, and carbon dioxide levels in the blood. Acidosis (low pH) indicates poor oxygenation.
Lactate Levels: Elevated lactate can indicate anaerobic metabolism due to hypoxia.
Complete Blood Count (CBC):
Evaluate overall health and detect infections, anemia, and other abnormalities that may contribute to or result from HIE.
Electrolytes and Metabolic Panel:
Assesses for imbalances that could exacerbate or result from the hypoxic-ischemic event.
Imaging Studies
Cranial Ultrasound:
Often the first imaging modality is used due to its safety and accessibility.
Can identify gross structural abnormalities, hemorrhage, or edema.
Magnetic Resonance Imaging (MRI):
MRI with Diffusion-Weighted Imaging (DWI): Highly sensitive in detecting early brain injury, often within the first few days of life.
Provides detailed images of brain structure and can identify specific areas of injury, helping to assess the extent and severity of HIE.
Magnetic Resonance Spectroscopy (MRS):
Complements MRI by assessing the metabolic status of brain tissues.
Helps detect metabolic abnormalities associated with hypoxic injury.
Electroencephalography (EEG)
Continuous Video EEG Monitoring:
Monitors brain activity for seizures and evaluates overall brain function.
Can help determine the severity of encephalopathy and guide treatment decisions.
Amplitude-Integrated EEG (aEEG):
Simplified version of EEG used for continuous monitoring in the neonatal intensive care unit (NICU).
Useful for early detection of seizures and assessing the severity of brain injury.
Additional Diagnostic Tools
Echocardiogram:
Evaluate heart function and detect congenital heart defects that might contribute to or result from HIE.
Umbilical Cord Blood Analysis:
Tests blood gases and pH from the umbilical cord at birth, providing immediate information about the newborn’s oxygenation status at delivery.
Early Interventions and Follow-Up
Once HIE is suspected or diagnosed, immediate interventions such as therapeutic hypothermia (cooling therapy) can be initiated to reduce the extent of brain injury. This treatment is most effective when started within six hours of birth.
Regular follow-up with pediatric neurology, developmental assessments, and continued imaging studies are crucial to monitor progress and manage any long-term effects of HIE.
Multidisciplinary care involving neonatologists, neurologists, physical therapists, and other specialists is often necessary to support the infant’s development and address any complications